

Clinical Resources
Power Adjustable Seat Height:
It’s Not Only Reasonable. It’s Necessary.
[PDF version of this page]
Wheelchair mobility is often only considered from the perspective of people moving from one point to another on a twodimensional plane. Vertical movement is necessary in order for people to function and participate in a three-dimensional world. A common intervention that provides vertical mobility within a wheelchair is a seat-elevating device.1 Hence, the provision of a power adjustable seat height (PASH) system is medically necessary to:
- Enable transfers across unequal surface heights
Transferring from a wheelchair to other surfaces such as a bed, toilet, or other surface is a necessary part of the daily routine. Transferring is a means to accomplish MRADLs (Mobility Related Activities of Daily Living), and therefore it is considered a medical necessity.1 - Adjust the seat height slightly above the surface to be transferred to/slightly below the surface to be transferred from, or
- Adjust the seat height equal to the surface to be transferred to/from in order to:
- Compensate for Lower Extremity (LE) weakness
- Compensate for Upper Extremity (UE) weakness and/or limited range of motion
- Compensate for joint or muscle pain in the neck, back, UEs or LEs
- Minimize the resistance of gravity when attempting to transfer uphill
- Compensate for balance challenges at rest or when moving

Kiel
Kiel has sustained an incomplete spinal cord injury at the C5/6 level. He has impaired sensation below the level of injury. He presents with good/normal strength in his shoulders and elbow flexor (bending) muscles, fair to good strength in the elbow extensor (straightening) muscles, fair strength in the wrist flexors and extensors and fair grasp. He has poor to fair sitting balance as he is unable to sit without using his upper extremities or postural support systems for assistance.
A wheelchair user is more readily able to transfer in a downhill direction using a sliding board versus uphill or to a level surface. In the downhill direction gravity assists as opposed to providing additional resistance and difficulty, as in the uphill direction. Transferring in a downward direction requires less upper extremity strain.1

From a static seat height of 21” Kiel is unable to transfer to his bed at a height of 23” using any method and is dependent on a personal care attendant (PCA).

Kiel loses his balance (photo above) during the transfer from his bed at 23” high to his wheelchair at a static height of 21” as the height differential is too great and the force of gravity is too strong. This places him at high risk for injury from a fall without the support of a PCA.
To independently transfer from his bed to the wheelchair with his sliding board, Kiel adjusts the wheelchair seat height to 22” (not shown). This allows him to utilize gravity effectively to assist with the transfer without putting him at heightened risk for an adverse occurrence or the need for an aide.
Kiel adjusts the wheelchair seat to several different heights throughout the day depending on whether he is transferring to or from the toilet or in/out of his shower commode chair for bathing. Without this capability he requires the services of a PCA for a minimum of 2 hours per day for transfers. At a median salary of $10/hour2 use of a PASH system saves $7,300 in PCA services per year or $36,500 over the 5-year reasonable useful lifetime of the equipment.

With the seat elevated to 24” Kiel is able to perform an independent sliding board transfer to his bed at 23” high.
Josh
Josh was diagnosed with Limb-Girdle Muscular Dystrophy at the age of 8. At age 25 he presents with poor strength in all 4 extremities and poor to fair core strength. He has poor sitting balance and does not have the ability to perform a sit-pivot or sliding board transfer. His standing balance is also poor and he is non-ambulatory; however, by standing with his hips and knees hyperextended he is able to “lock” the joints and use the structural integrity of his ligaments to do a stand-pivot transfer independently while holding on to the armrests of the chair.


Individuals with lower extremity weakness have difficulty assuming a standing position for transfers from a low seat to floor height. Rising from an elevated seat surface has been shown to require less lower-extremity strength and less extension momentum at the knees, ankles, and the hips.1
The use of a seat-elevating device to compensate for lower extremity weakness can assist with transfers, therefore prolonging independence.1
Regardless of whether he is in his own apartment or in his old room at his parent’s house, with the wheelchair seat elevated to 31”, Josh is still able to perform a stand-pivot transfer independently to and from his bed, which is also elevated to 31”. At any lower seat height, he is fully dependent on a personal care attendant to transfer.
Josh also remains fully independent in managing his bladder needs as he is able to stand from his wheelchair at a seat height of 31” to use the toilet. Without this feature Josh would require a PCA for 15 hours at a cost of $150 per day. The PASH feature “pays for itself” in less than 3 weeks.
In addition, Josh continues to use his ability to stand briefly to relieve pressure on the seated surface and minimize his risk for the development of pressure ulcers. He has full sensation and is aware of when he needs to perform a pressure relieving technique, However, without a PASH system he is unable to execute this, placing him at heightened risk for a pressure ulcer and costly medical care.
In the US, pressure ulcer care is estimated to approach $11 billion (USD) annually, with a cost of between $500 (USD) and $70,000 (USD) per individual pressure ulcer.3
- Enable performance/participation in Mobility Related Activities of Daily Living (MRADLs) such as bathing, dressing, feeding, grooming and toileting in the customary locations of the home.
- Adjust the vertical position of the seat to facilitate reach and:
- Compensate for UE weakness and/or limited range of motion
- Compensate for pain in the neck, back or UEs
- Compensate for balance challenges at rest or while moving
- Adjust the vertical position of the seat to facilitate reach and:





For individuals with limited reaching abilities, a seat-elevating device may be necessary for access to objects and surfaces within their home, thus improving their independence and decreasing their dependence on others.1
For Kiel, who lives alone, “feeding” as a MRADL comprises all aspects of meal preparation including, but not limited to shopping for groceries, putting the groceries away, cooking the meal, eating and cleaning up afterwards. He is fully independent in all aspects of the essential, life sustaining activity of obtaining nutrition and hydration as he has full access to the vertical environment with the use of a power adjustable seat height system. The inability to reach and function safely in the kitchen or lack of adequate access to food and water puts Kiel at heightened risk for preventable and costly secondary medical complications.
Without this power seat option, Kiel would be rendered dependent on an unnecessary personal care attendant for an additional hour each day. At a median salary of $10/hour2 this adds an additional $3,650 to the cost of PCA services annually, or $18,250 over the 5-year reasonable useful lifetime of the equipment.
A power adjustable seat height system supports access to all areas of the home necessary for completion of, or participation in, MRADLs at the highest level of function possible. By adjusting the height of the seat along the vertical continuum, to the height necessary to complete the task, the beneficiary increases the biomechanical advantage of the upper extremities to:
- Maximize strength of available muscles by changing arm leverage
- Maximize available range of motion at the shoulder, elbow and wrist
- Minimize damage/injury to the UEs
- Reduce the load when reaching for, picking up, lifting or carrying items
- Decrease over-shoulder/overhead reaching activities, minimizing over-use injuries
- Maintain and/or improve seated position
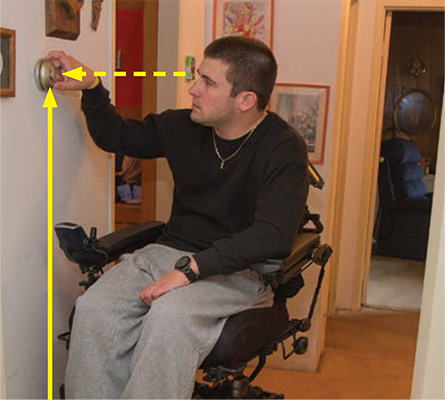
Kiel experiences thermoregulatory dysfunction secondary to his spinal cord injury (SCI). Thermoregulation is the process that allows the human body to maintain its core temperature. Thermoregulatory dysfunction in individuals with SCI refers to the fact that their body cannot perform this function properly. As a result, Kiel needs to be able to adjust the thermostat independently for his health and safety.
While he can reach the thermostat at a height of 48” from a low, static seat height, he is unable to see what temperature he has adjusted it to without the capability of adjusting the height of his wheelchair seat. Vertical adjustment provides him the visual access he needs to support his reaching activity, independently manage this condition and not incur additional medical costs from an adverse occurrence.

To perform all aspects of the dressing MRADL, Kiel must be able to access the clothes hangers at 65” as well as the closet shelves at 68”.

Health Services Research estimated that 13.2 million non-institutionalized adults receive an average of 31.4 hours of personal assistance in ADLs and IADLs per week.4 For Kiel use of a PASH system allows him to function safely and independently in his own home without the need for any PCA services. This feature saves $314/week, $16,328/year or $81,640 over the 5-year reasonable useful lifetime of the power adjustable seat height system.
Seat elevators may also help reduce upper extremity pain and help delay secondary complications to the shoulders. Studies have found an association between overhead activity and the development of shoulder pain and shown that the degree of upper arm elevation is one of the most important parameters influencing shoulder muscle load. When reaching from an elevated position, these loads are reduced, which is significant for individuals with already compromised upper extremity strength and range of motion.1
Madonna
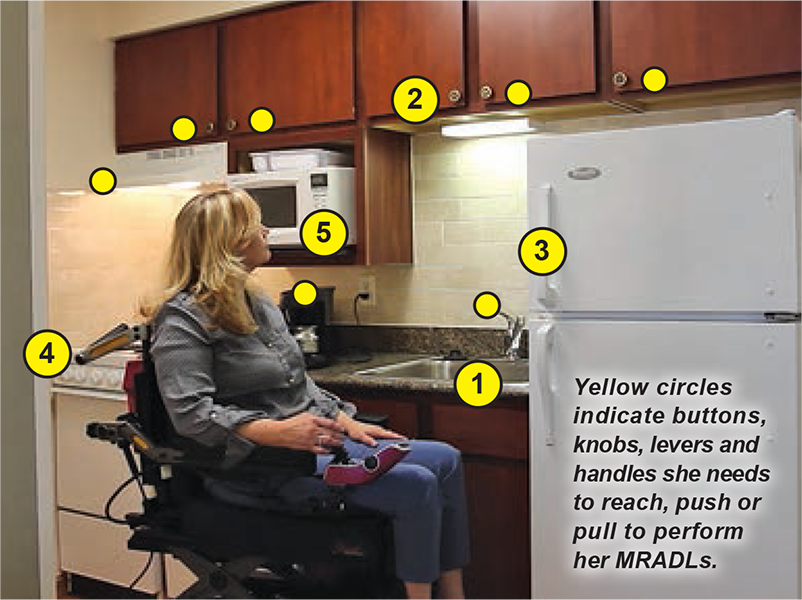
Either by building code, or conventional design, we know the average height of the surfaces and areas Madonna must be able to reach to perform or participate in all of her mobility-related activities of daily living without heightened risk for injury or an adverse occurrence.
- Counter top height = 36” (48” to coffee pot)
- Kitchen upper cabinet height = 54” at bottom, 84” at top
- Freezer height = 50” - 72”
- Stove top height = 36” (42” with a 6” pan)
- Over stove microwave height = 54” at bottom, 66” at top

Madonna sustained an incomplete spinal cord injury at the T10 level at age 18. She used a manual wheelchair for 35 years but at 53, as she ages with a disability, she is experiencing significant pain and strength limitations in her neck, shoulders and upper back from overuse injuries. As a single parent, she found herself reaching overhead hundreds of times each day to cook, clean and do laundry from a low, static seat height, exacerbating her pain. In addition, she sustained third-degree burns twice while removing a hot, cooked item from the stove due to the poor biomechanical position of her upper extremities from a low seat height.
Medical care for Madonna may have been prevented by adjusting her wheelchair seat to the appropriate height for the task cost she was performing, thereby saving thousands of dollars for each occasion.
A study comparing the frequency and duration of overhead arm activity between wheelchair users and occupationally matched nonwheelchair users during an 8-hour workday found that wheelchair users performed an average of 297 episodes of overhead arm activity, while controls performed an average of 53 episodes.5 According to a number of studies, surgical treatment for rotator cuff tears can cost between $300 and $15,000 (hospital cost), and approximately $250 to $5,000 for surgeon fees. For Madonna, use of a power wheelchair with a PASH system is essential to the preservation of her upper limb function, safety and continued independence.

- Adjust the vertical position of the seat to improve the line of sight and:
- Reduce overextended neck position (hyperlordosis) that results from looking up
- Relieve strain/minimize pain at the neck, shoulders and upper back
- Enhance vision and/or visual access to the environment
When talking at eye level with others, typical hyperlordotic cervical curvatures of the spine can be reduced. This relieves strain on the neck and may help enhance vision, thus helping to prevent secondary complications.1 These complications may include, but are not limited to headaches, numbness/tingling in arms, muscle pain/fatigue, spondylosis, disk herniation/rupture and/or increased pressure at the fracture location for an individual with a spinal cord injury.
Jesse



Jesse sustained a complete spinal cord injury at the C3/4 level. He has no sensation or movement below his level of injury and as a result drives his power wheelchair with a head array drive control system. In a wheelchair with a low, nonadjustable seat, Jessie assumes a hyperlordotic position of his head and neck as he attempts to communicate his care needs to a caregiver. As a result, he falls forward in the chair, thereby losing contact with the drive control system. This position also significantly reduces his respiratory capacity, rendering him unable to communicate and places him at high risk for a severe adverse respiratory event if his loss of position in the chair goes unnoticed, even briefly.
With the seat elevated along the continuum, Jesse is able to maintain his postural alignment, including a good position of his head and neck, to reduce strain at the fracture site, promote an open airway, and contact with his drive control system at whatever height he requires throughout the day to participate in his MRADLs.
An elevating seat may also allow a person in a wheelchair to hear and engage in conversations within a noisy environment, as well as to see and navigate more safely through a crowd of people.1
Zoe


Zoe was born with Tetra-Amelia Syndrome, a rare genetic disorder characterized by the absence of all four limbs. She drives her chair with a chin control device in the elevated position to improve her line of sight for safe operation in navigating her environment. However, to engage in communication with her caregivers and others, there are times when she is fully elevated or partially elevated and there are times when she is down in the lowered position, depending on the situation. This allows her to maintain her balance in the chair, remain in contact with her drive control device, and participate in her mobility-related activities of daily living as well as her education.
A power adjustable seat height system is a reasonable accommodation that enables her to have an equal opportunity to participate in her education and ultimately be considered for employment.



- Adjust the vertical position of the seat to augment safety and:
- Compensate for respiratory compromise
- Compensate for non-reducible postural deformities
- Repress muscle spasticity and/or reflex activity that causes involuntary movement
Mark

Mark was born with Cerebral Palsy. He is fully independent in all his activities of daily living at the wheelchair level even though he presents with spasticity in all 4 extremities and displays a significant postural deformity (note the curvature of his spine) when sitting. When Mark looks up from a low, seated position he exhibits an STNR (Symmetric Tonic Neck Reflex) that triggers spasticity and involuntary movement that results in him flexing his legs and extending his arms. This causes him to lose his positioning in the wheelchair, and appropriate contact with his postural supports, which can result in injuries. It also increases his risk for the development of pressure ulcers on the seated surface due to shearing forces. In addition, it negatively impacts his ability to reach and function to perform his mobility related activities of daily living.
Conclusion...
It is RESNA’s position that seat elevators are often medically necessary for wheelchair users by enabling them to reach, improving MRADL abilities, facilitating or enabling transfers, providing peer height at different ages, enhancing independence and productivity and delaying or preventing pain and secondary complications of the upper extremities [and neck].1
It is our position that power wheelchairs provide 360° of movement in a two dimensional plane, but we live in a three dimensional world. The addition of a highly functional power adjustable seat height system is medically necessary to raise and lower the client in their seated position, without changing the seat angle(s), to provide changes in vertical position and access to the environment for transfers, reach, communication and an accurate line of sight to perform or participate in MRADLs (Mobility Related Activities of Daily Living).


1Arva, J. et al, (2009). RESNA Position on the Application of Seat-Elevating Devices for Wheelchair Users. Assistive Technology, 21(2), 69-72. http://doi:-10.1080/10400430902945587
2https://www.payscale.com/research/US/Job=Personal_Care_Attendant_(PCA)/Hourly_Rate
3National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance, Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler (Ed.) Cambridge Media; Osborne Park, Western Australia; 2014
4LaPlante, M.P., Harrington, C., Kang, T. (2002) Estimating Paid and Unpaid Hours of Personal Assistance Services in Activities of Daily Living Provided to Adults Living at Home. Health Services Research, 37(2):397-415. http://doi:10.1111/1475-6773.029
5Sabari, J., Shea, M., Chen, L., Laurenceau, A., Leung, E, (2016). Impact of Wheelchair Seat Height on Neck and Shoulder Range of Motion During Functional Task Performance. Assistive Technology, 28(3), 183-189. http://doi:10.1080/10400435.2016.1140692